CJR-X: The Complete Guide to CMS’s Proposed Nationwide Bundled Payment Model

What You Need To Know About CJR-X
CMS has proposed CJR-X — Comprehensive Care for Joint Replacement Expanded — a mandatory nationwide bundled payment model for hip, knee, and inpatient ankle replacements. If finalized, it will affect every eligible acute care hospital in the country beginning October 1, 2027.
This guide breaks down exactly how the model works, who is impacted, and what PRO data collection has to do with your hospital’s financial performance under it.
In this guide we cover:
- What CJR-X Is and Why It’s Coming: The proposed rule builds on the original CJR Model’s proven track record of reducing Medicare episode spending — and expands it nationwide.
- Who’s Affected: Any acute care hospital paid under IPPS and OPPS that performs hip or knee replacements should plan to participate. Limited exclusions apply.
- How Financial Accountability Works: Hospitals earn reconciliation payments for spending below their regional target price — or owe repayments if they exceed it. Two-sided risk applies from Performance Year 1.
- How Quality Determines Payment: A Composite Quality Score across five measures governs your effective discount factor. Falling below “Acceptable” means forfeiting all upside — even if you came in under budget.
- The Role of the THA/TKA PRO-PM: Patient-reported outcomes are now a mandatory, scored component of CJR-X — not a bonus. Here’s what that means for your program.
- Key Differences from the Original CJR Model: A side-by-side breakdown of what changed and what stayed the same.
- What Hospitals Should Be Doing Now: Practical steps to assess readiness before Performance Year 1 begins.
 Comprehensive Care for Joint Replacement – Expanded (CJR-X): Summary and Key Differences from the Original CJR Model
Comprehensive Care for Joint Replacement – Expanded (CJR-X): Summary and Key Differences from the Original CJR Model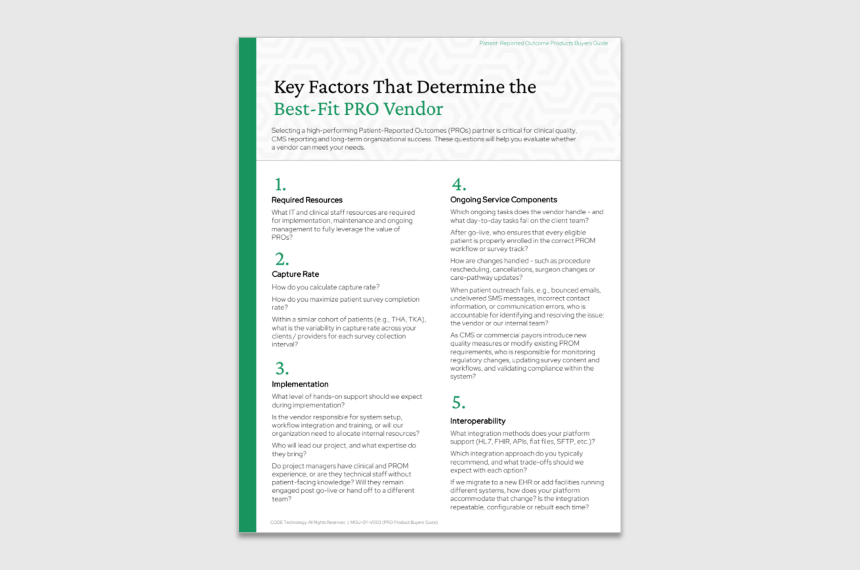 PRO Vendor Buyers Guide
PRO Vendor Buyers Guide CJR Simplified. A Practical Guide to Understanding & Preparing for CJR
CJR Simplified. A Practical Guide to Understanding & Preparing for CJR