
Overview of PROM Use in Robotic Colorectal Surgery
Colorectal surgery presents a highly heterogeneous than inguinal hernia repair from a PROM standpoint, because it spans multiple distinct procedure types — rectal cancer resection, colon cancer resection, IBD surgery — each with its own relevant domain of dysfunction. A systematic review of colorectal surgery PROMs from 2007–2018 identified 368 eligible studies using 165 distinct patient-reported outcome measures, with only 30 (18%) used five or more times and 102 (62%) used only once. PubMed Central.
This fragmentation is even more pronounced in the robotic-specific literature, where most studies still prioritize perioperative technical outcomes over standardized patient-reported outcome measures (PROMs).
The Most Commonly Used Disease-Specific PROMs by Procedure Category
Rectal Cancer Surgery (Most common robotic colorectal procedure)
1. LARS Score (Low Anterior Resection Syndrome Score) — Emerging as the dominant disease-specific PROM for robotic rectal surgery
The LARS score was developed as a patient-reported outcome measure to evaluate the severity of bowel dysfunction following rectal surgery by scoring the major symptoms of LARS: incontinence for flatus and liquid stool, frequent bowel movements, fragmentation/clustering of stools, and urgency. The higher the LARS score, the higher the level of QoL impairment, and severity is categorized at three levels: no LARS (0–20), minor LARS (21–29), and major LARS (30–42). PubMed
Studies using the LARS score to directly compare robotic and laparoscopic surgery have found that robotic surgery significantly reduced the incidence and severity of LARS in low rectal cancer patients compared with laparoscopic surgery, with LARS surveys conducted at 6, 12, and 18 months postoperatively. PubMed Central
The EORTC QLQ-C30 and QLQ-CR29 have been found to play a complementary role to the LARS score in evaluating quality of life for patients following both laparoscopic and robotic rectal cancer surgery, suggesting the two instruments address distinct but overlapping domains. Wiley Online Library
2. EORTC QLQ-CR29 (with QLQ-C30 core) — Most widely used cancer-specific QoL module
The EORTC QLQ-CR29 was developed to assess important issues such as bowel, bladder, and sexual dysfunction and problems relating to stoma formation in colorectal cancer patients. It is used in conjunction with the 30-item core EORTC QLQ-C30 questionnaire. Springer
The QLQ-CR29 contains 29 items presented on 4-point Likert scales, with four multi-item scales assessing urinary frequency, fecal seepage, stool consistency, and body image, plus single items assessing other common problems following treatment for colorectal cancer. Frontiers This pairing (QLQ-C30 + CR29) is the most commonly used PROM combination in robotic colorectal cancer studies in the European and Asian literature.
3. FACT-C (Functional Assessment of Cancer Therapy – Colorectal)
The FACT-C consists of 36 items presented on a 5-point Likert scale across four domains of well-being — physical, emotional, social, and functional — plus the Colorectal Cancer Subscale (CCS). Frontiers It is more commonly used in North American robotic colorectal studies.
4. MSK-BFI (Memorial Sloan Kettering Bowel Function Instrument)
The Memorial Sloan Kettering Cancer Center Bowel Function Instrument is among the dedicated LARS-related scores that have emerged in recent years, and strong correlations between it and the LARS score have been found, notably for the urgency and frequency subscales. Springer It is primarily used in high-volume cancer center robotic rectal series.
Fecal Incontinence Assessment (Post-sphincter-preserving surgery)
5. Wexner Score (Cleveland Clinic Florida Fecal Incontinence Score / CCIS)
The Wexner score, the St. Mark’s score, and the Fecal Incontinence Severity Index (FISI) are all validated instruments that assess the frequency of incontinence episodes; the Wexner score is the most widely used of the three despite being the least rigorously validated. PubMed Central
In robotic multiquadrant colorectal procedures including total proctocolectomy with IPAA, the Wexner score for fecal incontinence is frequently assessed at 3 months after ileostomy closure as the primary functional PROM. PubMed Central
6. FISI (Fecal Incontinence Severity Index)
Among the three fecal incontinence instruments, the scoring and validation of the FISI are the most methodologically rigorous. PubMed Central However, it appears less frequently than the Wexner score in robotic colorectal series specifically.
For IBD Surgery (Robotic colectomy, proctocolectomy with IPAA)
7. IBDQ (Inflammatory Bowel Disease Questionnaire)
The IBDQ-32 is the most frequently used instrument to capture disease-specific quality of life in randomized clinical trials for ulcerative colitis, assessing four domains: bowel symptoms (10 items), systemic symptoms (5 items), emotional function (12 items), and social function (5 items), on a 7-point Likert scale. MDPI
A systematic review found the IBDQ and its shortened version (SIBDQ) to be the most widely used PROMs for IBD-related colorectal surgery, with the SIBDQ potentially preferred due to lower response burden. PubMed Central
Key Findings on PROM Use in Robotic Colorectal Surgery
The robotic colorectal surgery literature — like the broader colorectal surgery PROM landscape — overwhelmingly uses generic QoL instruments (SF-36, EQ-5D) rather than disease-specific ones as primary endpoints. The notable exception is the LARS score, which has been explicitly deployed in robotic vs. laparoscopic comparative studies and is becoming the de facto standard disease-specific PROM for robotic rectal surgery outcomes. The EORTC QLQ-CR29 + C30 pairing is the most rigorously validated colorectal cancer-specific combination and is increasingly seen in higher-quality robotic series.
Comparison of Disease-Specific PROMs in Robotic Colorectal Surgery
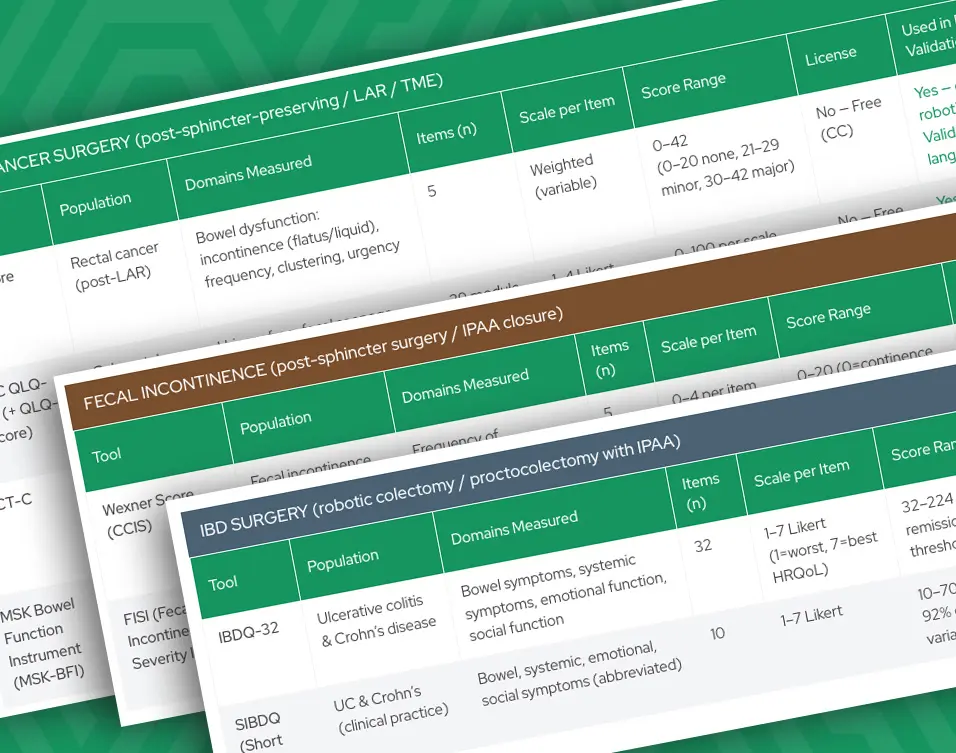
Given the wide variation in procedures and outcomes measured in colorectal surgery, PROM selection is highly dependent on clinical context. The chart below compares the most commonly used disease-specific PROMs across robotic colorectal procedures, including rectal cancer, fecal incontinence and IBD, highlighting what each tool measures, how it is scored, and where it is most commonly applied.
Patient-Reported Outcome Measures (PROMs) | da Vinci Robotic Colorectal Procedures | Organized by Indication
| Tool | Population | Domains Measured | Items (n) | Scale per Item | Score Range | License | Used in Robotic Surgery / Validation |
|---|---|---|---|---|---|---|---|
| LARS Score | Rectal cancer (post-LAR) | Bowel dysfunction: incontinence (flatus/liquid), frequency, clustering, urgency | 5 | Weighted (variable) | 0–42 (0–20 none, 21–29 minor, 30–42 major) |
No — Free (CC) | Yes — dominant PROM in robotic LAR studies | Validated in 24+ languages |
| EORTC QLQ-CR29 (+ QLQ-C30 core) | Colorectal cancer (colon & rectum) | Urinary freq, fecal seepage, stool consistency, body image, sexual/stoma fx, bowel sx | 29 module + 30 core = 59 total | 1–4 Likert (some 0–6) | 0–100 per scale (higher = worse sx or better fxn depending on scale) | No — Free (EORTC) | Yes — widely used in robotic rectal/colon cancer series; rigorous international validation |
| FACT-C | Colorectal cancer | Physical, emotional, social, functional well-being + Colorectal Cancer Subscale (CCS) | 36 | 0–4 Likert (0=not at all, 4=very much) | 0–144 (CCS subscale 0–40) | No — Free | Common in North American robotic CRC studies | Well validated |
| MSK Bowel Function Instrument (MSK-BFI) | Rectal cancer (post-LAR) | Frequency, dietary restrictions, urgency, soilage, social/psychological impact | 18 | 1–4 Likert | 18–76 (higher = better function) | No — Free | Used at high-volume cancer centers; strong correlation with LARS score |
| Tool | Population | Domains Measured | Items (n) | Scale per Item | Score Range | License | Used in Robotic Surgery / Validation |
|---|---|---|---|---|---|---|---|
| Wexner Score (CCIS) | Fecal incontinence (post-rectal surgery, post-IPAA) | Frequency of incontinence: solid, liquid, gas, pad use, lifestyle alteration | 5 | 0–4 per item (0=never, 4=always) | 0–20 (0=continence, 20=complete incontinence) | No — Free | Most used incontinence PROM in robotic colorectal series | Widely used; weakest validation of FI tools |
| FISI (Fecal Incontinence Severity Index) | Fecal incontinence | Frequency of FI episodes: gas, mucus, liquid, solid stool | 4 | Weighted 5-point frequency scale | 0–61 (0=no FI, 61=most severe) | No — Free | Less frequent than Wexner in robotic series; most rigorous validation of FI tools |
| Tool | Population | Domains Measured | Items (n) | Scale per Item | Score Range | License | Used in Robotic Surgery / Validation |
|---|---|---|---|---|---|---|---|
| IBDQ-32 | Ulcerative colitis & Crohn’s disease | Bowel symptoms, systemic symptoms, emotional function, social function | 32 | 1–7 Likert (1=worst, 7=best HRQoL) | 32–224 (≥170 = remission threshold) | No — Free | Most used IBD-specific PROM in robotic IBD surgery | Extensively validated globally |
| SIBDQ (Short IBDQ) | UC & Crohn’s (clinical practice) | Bowel, systemic, emotional, social symptoms (abbreviated) | 10 | 1–7 Likert | 10–70 (explains 90–92% of IBDQ variance) | No — Free | Lower respondent burden; suitable for clinical practice and office-based robotic follow-up |